KPV Peptide: Benefits, Dosage & Safety (2026 Guide)
KPV peptide is an anti-inflammatory tripeptide from alpha-MSH studied for gut, skin, and inflammation. A research guide to benefits, dosage, routes, and safety.


KPV peptide is a tripeptide made of lysine, proline, and valine that comes from the tail end of alpha-melanocyte-stimulating hormone (α-MSH). Researchers study it as an anti-inflammatory and antimicrobial agent that calms overactive immune signaling without shutting the immune system down. Most of the attention sits in three areas: gut inflammation, skin conditions, and whole-body inflammation driven by the NF-κB pathway.
One detail sets it apart from almost every other peptide. KPV is small enough to survive the digestive tract and get absorbed intact, so it can be taken by mouth. That is rare. It also explains why so much of the published work points at the gut.
This guide covers what KPV is, how it works, what the evidence supports, how it is dosed across injectable, oral, and topical forms, its safety profile, and the popular KPV plus BPC-157 pairing. A note on evidence before we start: the science here is preclinical. The findings come from cell cultures and animal models, not completed human clinical trials.
What is KPV peptide?
KPV is a fragment, not a full hormone. It is the last three amino acids of α-MSH, the sequence at positions 11 to 13, written as Lys-Pro-Val. Snip that tripeptide off the parent hormone and you keep most of the anti-inflammatory action while losing the pigment-darkening effect that α-MSH is known for. That trade is the whole appeal: calm without the tan.
The molecule is tiny, which matters more than it sounds. A three-amino-acid chain can ride into cells through the PepT1 transporter, a protein that normally shuttles small dietary peptides across the gut wall. Larger peptides get chewed up by digestive enzymes before they do anything. KPV slips through.
It also carries antimicrobial properties. Work going back to 2000 found that α-MSH and its C-terminal KPV sequence inhibit the growth of pathogens including Staphylococcus aureus and the yeast Candida albicans, with the lysine and proline residues doing most of that work (Cutuli et al., 2000).
Here is the quick profile:
Attribute | Detail |
|---|---|
Sequence | Lysine-Proline-Valine (Lys-Pro-Val) |
Parent molecule | Alpha-MSH, residues 11 to 13 |
Size | Tripeptide (three amino acids) |
Studied for | Gut inflammation, skin inflammation, systemic inflammation, wound healing |
Routes | Oral, subcutaneous injection, topical |
Evidence base | Preclinical (cell and animal models) |
How KPV works inside the cell
Most anti-inflammatory drugs work from the outside or blunt the immune system broadly. KPV does something different. It gets carried into the cell and switches off inflammatory signaling at the source.
The central target is NF-κB, a master switch that turns on genes for inflammation. In intestinal cells, nanomolar amounts of KPV blocked NF-κB activation and a second pathway called MAP kinase, which dropped the output of pro-inflammatory cytokines (Dalmasso et al., 2008). Fewer active inflammatory genes means less TNF-α and IL-6, two of the signals that drive redness, swelling, and tissue damage.
KPV reaches those cells through PepT1. That transporter sits in the small intestine and gets switched on in the colon during inflammatory bowel disease, so inflamed gut tissue is primed to pull KPV inside exactly where it is needed. Immune cells express PepT1 too, which gives the peptide a second route to the cells that fuel inflammation.
There is also a receptor angle. The parent hormone binds melanocortin receptors, especially MC1R, which appears on skin cells, immune cells, and more. KPV keeps some of that receptor activity, though research in colitis models found its benefit was at least partly independent of MC1R (Kannengiesser et al., 2008). In plain terms, it likely calms inflammation through more than one door.
The phrase researchers keep coming back to is "modulate, not suppress." KPV tones down excess signaling rather than disabling the immune response, so the body's normal defenses are meant to stay intact.

KPV benefits: what the research shows
The honest framing first. Every benefit below comes from laboratory and animal research. KPV has not been through the large human trials that would confirm these effects in people, so treat the following as research signals, not proven outcomes.
Gut health and IBD
This is the most studied use by a wide margin. In mouse models of colitis, oral KPV reduced the severity of disease triggered by both DSS and TNBS, two standard ways of inducing gut inflammation (Dalmasso et al., 2008). A separate team saw earlier recovery, better weight regain, and fewer inflammatory infiltrates in two different colitis models (Kannengiesser et al., 2008). The interest in Crohn's and ulcerative colitis grows directly out of this work.
A 2017 study pushed the delivery further. Researchers wrapped KPV in hyaluronic-acid nanoparticles and found it eased ulcerative colitis in mice at a dose roughly 12,000 times lower than free KPV, while speeding up healing of the gut lining (Xiao et al., 2017). That is a striking efficiency gain and a sign of where targeted formulations may go.
Leaky gut and the intestinal barrier
"Leaky gut" describes a gut lining that has become too permeable, letting through things that should stay in the intestine. Because KPV calms inflammation inside epithelial cells and the colitis studies showed healing of the mucosa, it is studied as a way to help restore barrier integrity. The repair of the gut lining seen in the nanoparticle work speaks directly to this.
Skin and inflammation
KPV's skin reputation rests on its parent hormone's biology. α-MSH and its KPV fragment inhibit TNF-α-driven NF-κB activity in human keratinocytes and dermal fibroblasts, the two main cell types in skin, without triggering pigmentation. Reviews of melanocortin peptides flag KPV and related fragments as candidates for inflammatory skin conditions and wound healing because the MC1R receptor sits on most skin cells (Böhm and Luger, 2019). This is the rationale behind topical and oral use for eczema, psoriasis, and dermatitis, though dedicated human trials for those conditions are not there yet.
Systemic inflammation
Since NF-κB sits at the center of inflammation throughout the body, KPV's ability to dampen it is studied beyond the gut and skin. By lowering cytokines like TNF-α and IL-6 at the cellular level, it is positioned as a general anti-inflammatory tool in research settings.
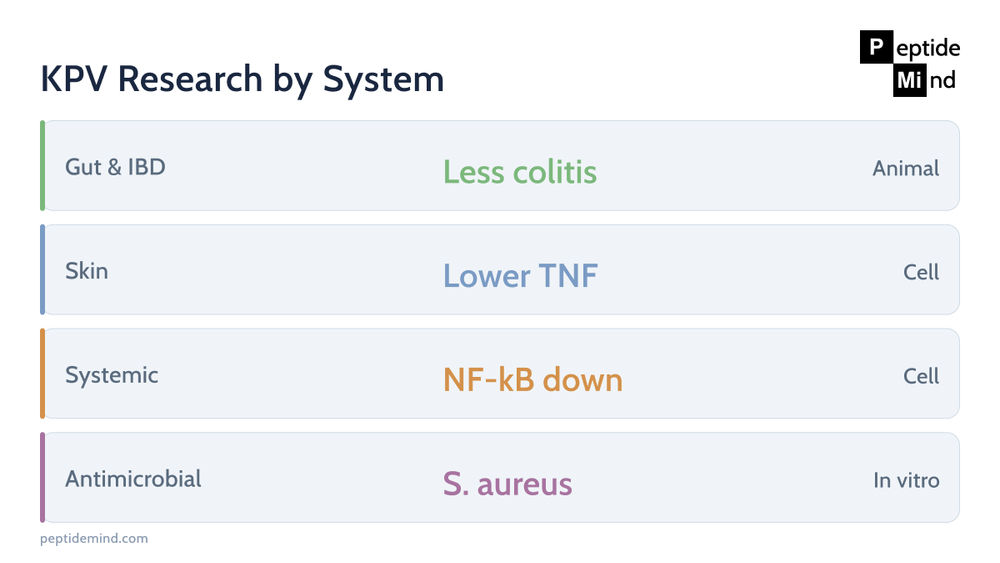
Research area | What studies report | Evidence level |
|---|---|---|
Gut and IBD | Less severe colitis, lower TNF-α and IL-6, faster mucosal healing | Animal and cell |
Intestinal barrier | Healing of the gut lining, PepT1 uptake into gut cells | Animal and cell |
Skin inflammation | Blocks TNF-α and NF-κB in keratinocytes and fibroblasts | Cell and preclinical |
Systemic inflammation | NF-κB and MAP-kinase suppression, cytokine reduction | Cell and animal |
Antimicrobial | Activity against S. aureus and C. albicans | In vitro |
KPV dosage: what the research and practitioners report
There is no established clinical dose for KPV, because the human trials that would set one have not happened. The numbers below come from preclinical scaling and from doses reported in practitioner and research-community settings. They are reference points, not prescriptions.
The range you will see most often is 200 to 500 mcg per day, with the exact figure depending on the route and the target.
Route | Commonly reported range | Most studied or used for |
|---|---|---|
Subcutaneous injection | 200 to 500 mcg per day | Systemic inflammation, broad use |
Oral (capsule or sublingual) | 250 to 500 mcg per day | Gut and IBD |
Topical | Compounded, varies by formula | Localized skin issues |
A few practical notes. Injectable KPV usually starts at the lower end and is held there for a stretch before any adjustment. Oral KPV leans on the PepT1 pathway, which is why it is favored for gut-focused research. Timing questions come up a lot; KPV does not have a strict morning-or-night requirement in the literature, so consistency matters more than the clock.
If you are working with a lyophilized (freeze-dried) injectable form, it has to be mixed before use. Our peptide reconstitution guide walks through the solvent, the math, and storage, and the peptide dosage calculator turns your vial size and target dose into exact units to draw.
Oral, injectable, or topical: choosing a route
KPV is one of the few peptides where the oral form is taken seriously, and that shapes the whole decision.
Oral KPV makes sense when the target is the gut. The peptide is stable enough to reach intestinal tissue, and PepT1 expression climbs in inflamed bowel, so the delivery and the problem line up. Capsules and sublingual sprays are the usual formats.
Injectable KPV, given subcutaneously, is the route for systemic goals where you want the peptide in circulation rather than concentrated in the gut. It is the most flexible option for general anti-inflammatory research use.
Topical KPV targets a specific patch of skin. For a localized flare of eczema or a slow-healing wound, applying it directly puts the peptide where the inflammation is without sending it body-wide.
The short version: gut points to oral, skin points to topical, and everything systemic points to injection. Many research protocols combine routes, for instance oral for the gut alongside topical for a skin issue.
Side effects and safety profile
KPV reads as well tolerated in the preclinical record. Animal studies have not flagged major toxicity, and the nanoparticle delivery paper described its carrier materials as generally recognized as safe (Xiao et al., 2017). Because the peptide modulates inflammation rather than suppressing immunity outright, it is not expected to leave users open to infection the way broad immunosuppressants can.
That said, the safety picture has real limits:
No human safety trials. The clean profile comes from animals and cells. Long-term effects in people are unknown.
Injection-site reactions. As with any subcutaneous peptide, redness, swelling, or irritation at the site can occur. Sterile technique lowers the risk.
Purity is a variable. Research-grade KPV is not regulated like a drug. An impure or mislabeled product carries more risk than the peptide itself, which is why a certificate of analysis matters.
Unstudied populations. KPV has not been evaluated in pregnancy, breastfeeding, or in people on immune-modifying medication. Those groups sit outside the evidence entirely.
Who should be most cautious? Anyone pregnant or nursing, anyone managing an autoimmune condition or taking immunosuppressants, and anyone with a known peptide allergy. The "who shouldn't take it" question does not have a clean research answer, so the conservative reading is that unstudied means unknown.
The KPV and BPC-157 stack
The most common pairing puts KPV next to BPC-157, and the logic is complementary rather than redundant. KPV calms inflammation. BPC-157 is studied for tissue repair, blood-vessel growth, and protection of the gut lining. One quiets the fire; the other rebuilds what the fire damaged.
For gut research in particular, the overlap is tidy. Both compounds have a body of preclinical work in the digestive tract, so a protocol aimed at the gut lining often reaches for both. The same pairing shows up in healing and recovery contexts for the same reason.
Compound | Primary research role | Contribution to the pair |
|---|---|---|
KPV | Anti-inflammatory (NF-κB) | Lowers inflammatory signaling |
BPC-157 | Tissue repair and GI protection | Rebuilds and protects tissue |
A caveat worth stating plainly: there is no human trial of the two together. The rationale is mechanistic, drawn from what each peptide does on its own. If you want to go deeper, our BPC-157 research guide covers that peptide in full, and KPV also appears alongside GHK-Cu, BPC-157, and TB-500 in the four-part KLOW blend; that KPV fraction is the only thing separating KLOW from the three-peptide GLOW blend, which our KLOW vs GLOW comparison sets out side by side. The related Wolverine stack pairs BPC-157 with TB-500 for a recovery-first protocol.

Is KPV legal? Research status in 2026
KPV is sold and studied as a research compound. It is not an approved drug, and it has not cleared the FDA process for treating any condition. In the United States, peptides like KPV, BPC-157, and TB-500 have drawn regulatory attention, and their compounding status has been under review, so the supply landscape can shift. In practice, that means KPV occupies a research-use space, quality varies between suppliers, and third-party purity testing is the buyer's main protection. Looking for a certificate of analysis is the single most useful habit.
Frequently asked questions
What are the benefits of KPV peptide?
In research, KPV is studied for calming gut inflammation (including colitis models linked to Crohn's and ulcerative colitis), supporting the intestinal barrier in leaky-gut contexts, easing inflammatory skin conditions like eczema and psoriasis, lowering systemic inflammation through the NF-κB pathway, and fighting certain microbes. All of these come from preclinical work rather than human trials.
Is KPV the safest peptide?
KPV has a clean preclinical safety record and modulates inflammation instead of suppressing immunity, which is why it gets called gentle. "Safest" overstates it, though, because there are no long-term human safety studies. It looks well tolerated in animals; that is not the same as proven safe in people.
What are the long-term effects of KPV peptide?
Unknown. The research runs short-term in cells and animals, so there is no reliable data on what months or years of use do in humans. Anyone using it should treat the long-term picture as an open question.
Who shouldn't take KPV peptide?
KPV has not been tested in pregnancy, breastfeeding, or in people on immune-modifying drugs, so those groups fall outside the evidence and have the most reason for caution. The same goes for anyone with a peptide allergy. Because the human data is missing, "unstudied" is the operative word.
Should KPV be taken in the morning or at night?
The research does not pin KPV to a specific time of day. Consistency from day to day matters more than whether you take it in the morning or the evening.
Can KPV help with eczema or psoriasis?
The mechanism fits, since KPV blocks the inflammatory signaling behind those conditions and its parent hormone is active in skin. But the support is preclinical and based on cell studies and melanocortin biology, not human dermatology trials. It is a research signal, not a settled treatment.
The bottom line
KPV peptide is a small, mechanistically interesting fragment of α-MSH with a real preclinical track record in gut inflammation, skin inflammation, and NF-κB-driven processes, plus an unusual ability to work orally. The mechanism is well mapped. The animal data is consistent. What is missing is the human trial layer that would turn a promising research compound into a proven therapy. Read the literature for what it is, keep an eye on purity, and treat the dosing figures as reference points rather than rules.
References
Dalmasso G, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008. https://pmc.ncbi.nlm.nih.gov/articles/PMC2431115/
Xiao B, et al. Orally targeted delivery of tripeptide KPV via hyaluronic acid-functionalized nanoparticles efficiently alleviates ulcerative colitis. Molecular Therapy. 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5498804/
Kannengiesser K, et al. Melanocortin-derived tripeptide KPV has anti-inflammatory potential in murine models of inflammatory bowel disease. Inflammatory Bowel Diseases. 2008. https://pubmed.ncbi.nlm.nih.gov/18092346/
Cutuli M, et al. Antimicrobial effects of alpha-MSH peptides. Journal of Leukocyte Biology. 2000. https://pubmed.ncbi.nlm.nih.gov/10670585/
Böhm M, Luger T. Are melanocortin peptides future therapeutics for cutaneous wound healing? Experimental Dermatology. 2019. https://pubmed.ncbi.nlm.nih.gov/30661264/
Disclaimer: This article is for educational and informational purposes only and describes preclinical and laboratory research. KPV is a research compound; it has not been approved by the FDA for the prevention or treatment of any disease, and nothing here is medical advice. Consult a licensed healthcare provider before making any health-related decisions.
Add a comment
This will be publicly visible.
Your email address will not be published.
Your comment will be reviewed by an admin before it is published.